Diagnosis + Treatment
The Big Picture
Dr. Jekyll and Mr. Hyde? [ Video ]
Five Dimensions of Human Personality
Think It's BPD but How Can I Know?
DSM Criteria for Personality Disorders
Treatment of BPD [ Video ]
Getting a Loved One Into Therapy
Top 50 Questions Members Ask
Home page
Forum
List of discussion groups
Making a first post
Find last post
Discussion group guidelines
Tips
Romantic relationship in or near breakup
Child (adult or adolescent) with BPD
Sibling or Parent with BPD
Boyfriend/Girlfriend with BPD
Partner or Spouse with BPD
Surviving a Failed Romantic Relationship
Tools
Wisemind
Ending conflict (3 minute lesson)
Listen with Empathy
Don't Be Invalidating
Setting boundaries
On-line CBT
Book reviews
Member workshops
About
Mission and Purpose
Website Policies
Membership Eligibility
Please Donate
June 10, 2026, 03:50:27 AM
Welcome,
Guest
. Please
login
or
register
.
Did you miss your
activation email?
1 Hour
5 Hours
1 Day
1 Week
Forever
Login with username, password and session length
Board Admins:
Kells76
,
Once Removed
Senior Ambassadors:
SinisterComplex
Help!
Boards
Please Donate
Login to Post
New?--Click here to register
Survey: How do you compare?
Adult Children Sensitivity
67% are highly sensitive
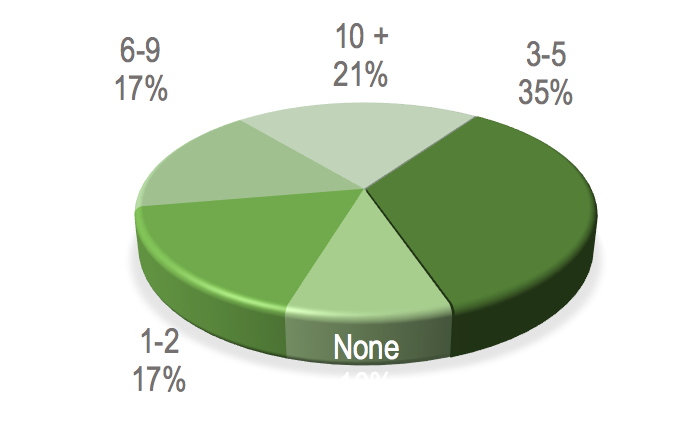
Romantic Break-ups
73% have five or more recycles
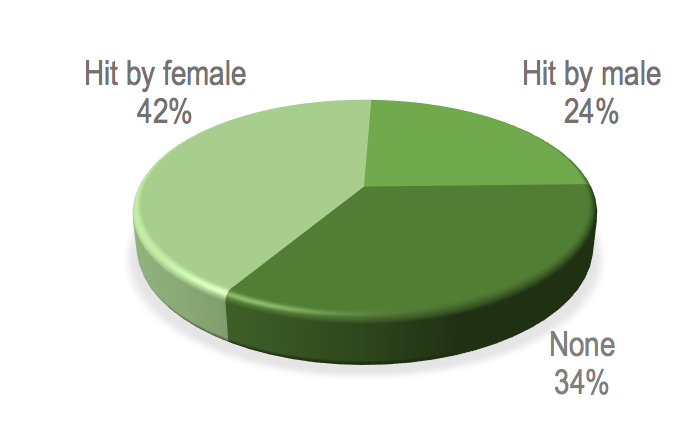
Physical Hitting
66% of members were hit
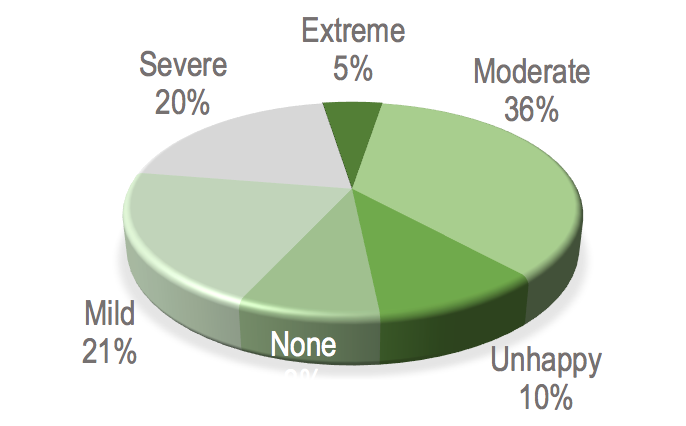
Depression Test
61% of members are moderate-severe
108
BPDFamily.com
>
Relationship Partner with BPD (Straight and LGBT+)
>
Romantic Relationship | Detaching and Learning after a Failed Relationship
> Topic:
BPD? Anxiety? CPTSD?
Pages: [
1
]
Go Down
« previous
next »
Print
Author
Topic: BPD? Anxiety? CPTSD? (Read 5712 times)
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
BPD? Anxiety? CPTSD?
«
on:
May 25, 2024, 03:37:55 AM »
I'm trying to figure out which of these an ex had, if not more than one.
When I met her, she told me she'd been diagnosed with anxiety. Later, she switched therapists, and this one said CPTSD. Toward the end of our time together, she seemed to be seeing yet another therapist, and this one thought BPD might be at work (and some paperwork she showed me also noted this).
I know it's tough for therapists to diagnose any of these issues, and there can be comorbidities, but her behavior could get pretty extreme and included:
1) Frequent lying, even about sometimes trivial things. She once admitted she lied all the time, often without even knowing why.
2) Poor memory, both in terms of life events and even sometimes recognizing familiar places and people.
3) Changes in voice, gestures, and even facial expressions. She always has a kind of Marilyn Monroe-ish voice, but it can deepen at times. And with changes in expression come changes in demeanor, to the degree it can seem like a completely different person.
4) Pseudoseizures and abrupt mood shifts. She was also diagnosed with ADD and on several daily medications, including antidepressants and antipsychotics (for the pseudo seizures).
5) Outbursts of anger. She once got furious with me for being late due to unavoidable road construction, for example. She was inexplicably angry at a neighbor who only seemed to be trying to be nice to her.
6) Suddenly breaking up for no apparent reason. One time while shopping, I'd made an innocent comment to her, which wasn't critical in any way. We parted happily, but by the time she got home, she called to tell me we couldn't see each other anymore because I'd hurt her feelings so bad.
7) Outpatient hospitalization for self harm or suicide ideation. She'd apparently attempted suicide years before I met her. When she got extremely stressed, she'd sometimes strike herself on the head. She could get incontinent.
8) Drug abuse (weed) and drug dealing (selling Adderall or some of the oxy she got prescribed for chronic pain). When she drank, she could be flirty and touchy-feely with strangers.
9) Bouts of extreme spending and making grandiose, unrealistic goals for the future.
10) Weirdly inappropriate comments, like telling me once how proud she was of her child's -- her words -- impressive genitalia.
11) Needing to be the damsel that would call at odd hours for rescue (ran out of gas, car won't start, etc.) even when she wasn't really in trouble.
12) Cheating. She told me she'd cheated in every relationship she'd ever had and had been married twice (at the time -- she might well be married again). While we were seeing each other, I caught her at her ex's or her ex at her place a few times, though in fairness I can't say I literally saw them together. Nonetheless, she alternated between saying she'd cheated on me and denying it. Whenever we broke up, she was back with the ex.
These are not the only things, but they're obviously a pretty healthy (or unhealthy) list. She'd also been a stripper (or so she said -- that was before I met her). Now, I don't hold dancing for a living against a woman, but it's sex work (if only marginally to some), and that seems to attract women with issues like BPD rather than, say, anxiety. She also claimed to have been physically and sexually abused as a child by family and later raped by strangers.
Keep in mind I discovered all of this over time, as we actually saw each other on and off over a period of years.
We'd get together, do okay for a while, I'd see red flags, then things would go south, and I'd break it off. Then she'd come at me like a Mack truck, insisting it would be different/she was getting help/I was the only one, etc.
To me, her behavior seems pretty classic BPD, at least based on what I've read. But then she showed me hospital paperwork with the other diagnoses. I've heard therapists sometimes diagnose BPD instead with, say, CPTSD both for stigma and insurance reasons.
So, what's it sound like to those of you with more experience?
P.S., Some may be asking why I want to know. Well, though that's really my business, no offense, some of it has to do with sorting all this out. For instance, I now know someone else with anxiety and wonder if I'll see the same patterns repeating themselves (though we're not romantically involved nor do I expect us to be).
What I wonder, too, is what the prognosis is for someone with this degree of issues, even with therapy and medication.
Thanks.
Logged
jaded7
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Romantic partner
Relationship status: unclear
Posts: 592
Re: BPD? Anxiety? CPTSD?
«
Reply #1 on:
May 25, 2024, 11:26:44 AM »
There's a current thread on the 'divorcing' board on this subject as well. One of the admins posted a link to an older
discussion of this question you might find helpful.
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #2 on:
May 25, 2024, 05:25:04 PM »
There's still considerable debate in the research literature on the relationship between cPTSD and BPD, and features that distinguish each. As you note, there is a lot of comorbidity. I myself qualify for a diagnosis of cPTSD, but would never qualify for a diagnosis of BPD. Some of the symptoms you list for your ex really leave me thinking BPD.
In case you might find it helpful, here's some material from recently published studies:
"While BPD and CPTSD do exhibit overlap in the type of difficulties across affect regulation, self-concept, and interpersonal relationships, there are also important distinctions that are reflected in how symptoms manifest for either CPTSD or BPD. For example, in CPTSD, there is a persistent negative sense of self, while in BPD there is an unstable sense of self that can be internalizing or positive and may change back and forth between the two. Interpersonal difficulties in CPTSD are often characterized by avoidance and disconnection, while in BPD, they may include relationships marked by either ongoing or intermittent volatility and by efforts to connect with others to avoid feelings of abandonment (Cloitre et al., 2014). BPD is also marked by more extreme strategies to regulate affect. For example, suicidal or self-harming behaviors often result from attempts to escape from or change emotions that seem intolerable (Conklin et al., 2006)."
"...These relationships with external correlates may be useful in identifying key features of each disorder that distinguish them from one another despite their substantial overlap, such as angry outbursts more often amounting to aggression or violent behavior in BPD compared to CPTSD (ICD-11 PTSD and DSO) or pervasive attempts to avoid internal and external trauma stimuli in CPTSD (ICD-11 PTSD and DSO) compared to BPD."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9107503/
"Overall results indicate that the distinction between BPD and CPTSD symptoms was strongly supported. However, our results also suggest that two symptoms of CPTSD, namely, “When I am upset, it takes me a long time to calm down.” (AD1) and “I feel numb or emotionally shut down” (AD2), were the only symptoms connecting the BPD with CPTSD constructs and potentially contribute to the overlap of the two conditions (Powers et al., 2022; Frost et al., 2020)."
https://www.researchgate.net/publication/366964802_Borderline_Personality_Disorder_BPD_and_Complex_Post_Traumatic_Stress_Disorder_CPTSD_A_network_analysis_in_a_highly_traumatised_clinical_sample
"...the DSO [Disturbances of Self-Organization] symptoms of cPTSD are consistent with the flight response, which is characterized by both unmodulated distress (i.e., DSO’s difficulty in self-calming, guilt, and sense of worthlessness) and both conscious and unconscious attempts to escape from further harm (i.e., DSO’s emotional numbing and relational detachment). Flight responses involve active attempts to restore safety by disengaging from sources of harm (e.g., fear of closeness) and distress, which are highly self-referential (i.e., associated with the DMN [Default Mode Network]) and include attempts to mobilize executive problem solving and decision-making (i.e., associated with the PfC [prefrontal cortex]). Thus, cPTSD could be understood as the maladaptive persistence of initially adaptive stress reactions that progress from hypervigilance (i.e., PTSD) to emotional/relational shut-down (i.e., DSO).
BPD could emerge as a fight response when executive control capabilities are not sufficient to sustain PTSD’s freeze/hypervigilance and cPTSD’s flight/detachment, which is consistent with evidence of diminished connectivity within the salience network and the DMN, and hypoactivation of the PfC plus hyperactivation of the amygdala, in BPD. Instead of attempts to cope by means of vigilance or detachment, BPD involves reacting in a fight mode with impulsive, disorganized, and hostile behavior in relationships and limited or no sense of self-awareness and self-efficacy. The fight reaction characterizing BPD includes a surge in bodily arousal initiated by the brain’s innate alarm system [102], and desperate attempts to prevent or retaliate for perceived or real abandonment. The alternating enmeshment in and rejection of relationships characterizing BPD also is consistent with the emotional dysregulation and deficits in executive function that have been found to occur among individuals who are experiencing disorganized attachment."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8103648/
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #3 on:
May 25, 2024, 08:33:32 PM »
P.S. re: "what the prognosis is for someone with this degree of issues, even with therapy and medication."
I'll just comment here regarding BPD, since that seems the more relevant construct in this case.
BPD can be successfully treated. On the BPDfamily message boards, I have seen quite a lot of accounts of people who improved greatly. Certain structured therapies seem to have much greater efficacy for BPD than traditional psychotherapy. Traditional psychoanalysis "on the couch", using free-association, can sometimes cause BPD patients to deteriorate. Though even with appropriate evidence-based therapies, a substantial proportion of BPD patients show no improvement. Full recovery is possible (even in extreme cases), but appears relatively rare. Medications have very limited efficacy in treating BPD - though they can be used to ameliorate certain symptoms. But meds can't address the core problems.
DBT is the most widely used treatment for BPD. But a lot of BPD patients dislike it. Treatment dropout is frequent. I managed to engage my ex into DBT therapy, but she disliked it, showed little improvement over the course of a year and a half of therapy, and then dropped out.
Schema Therapy might currently be the most efficacious treatment for BPD. A network meta-analysis found its effect size (in reducing BPD symptoms) to be twice as large as other current BPD-specific treatments. Though that was based on a limited number of randomaized controlled trials - more research needs to be done. Schema Therapy also shows a lower patient dropout rate than other BPD therapies. One reason might be because in Schema Therapy, the therapist is often speaking to the "vulnerable child mode" in the patient (and is providing "limited reparenting"), rather than just speaking to the "adult", as in most therapies. Unfortunatetly, there are relatively few adequately trained practitioners providing Schema Therapy in the U.S., even though it was developed in the U.S. It's much more widely used in Europe and Australia.
Logged
Kashi
Offline
What is your sexual orientation: Gay, lesb
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 91
Re: BPD? Anxiety? CPTSD?
«
Reply #4 on:
May 26, 2024, 03:45:28 AM »
CPTSD has some similar traits as BPD, but it's varied depending on the individual and circumstance
What you are describing seems pure BDP to me
Anxiety can cover both BPD and CPTSD but it's a different beast.
You need to know "why"
Anxiety is so common now. From school age children all the way through. I think it's just what we as humans have come to know. Years ago we were told to suck it up take it so it wasn't spoken about.
Logged
EyesUp
Senior Ambassador
Offline
Gender:
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: divorced
Posts: 685
Re: BPD? Anxiety? CPTSD?
«
Reply #5 on:
May 26, 2024, 06:23:30 AM »
As others noted, there are some common co-morbidities, and some common features/attributes.
It does sound like your X has some b-cluster behaviors.
Ultimately, it’s up to her to accept or not accept any particular diagnosis or therapy…
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #6 on:
May 27, 2024, 12:55:28 AM »
Quote from: Pensive1 on May 25, 2024, 05:25:04 PM
There's still considerable debate in the research literature on the relationship between cPTSD and BPD, and features that distinguish each. As you note, there is a lot of comorbidity. I myself qualify for a diagnosis of cPTSD, but would never qualify for a diagnosis of BPD. Some of the symptoms you list for your ex really leave me thinking BPD.
In case you might find it helpful, here's some material from recently published studies:
"While BPD and CPTSD do exhibit overlap in the type of difficulties across affect regulation, self-concept, and interpersonal relationships, there are also important distinctions that are reflected in how symptoms manifest for either CPTSD or BPD. For example, in CPTSD, there is a persistent negative sense of self, while in BPD there is an unstable sense of self that can be internalizing or positive and may change back and forth between the two. Interpersonal difficulties in CPTSD are often characterized by avoidance and disconnection, while in BPD, they may include relationships marked by either ongoing or intermittent volatility and by efforts to connect with others to avoid feelings of abandonment (Cloitre et al., 2014). BPD is also marked by more extreme strategies to regulate affect. For example, suicidal or self-harming behaviors often result from attempts to escape from or change emotions that seem intolerable (Conklin et al., 2006)."
"...These relationships with external correlates may be useful in identifying key features of each disorder that distinguish them from one another despite their substantial overlap, such as angry outbursts more often amounting to aggression or violent behavior in BPD compared to CPTSD (ICD-11 PTSD and DSO) or pervasive attempts to avoid internal and external trauma stimuli in CPTSD (ICD-11 PTSD and DSO) compared to BPD."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9107503/
"Overall results indicate that the distinction between BPD and CPTSD symptoms was strongly supported. However, our results also suggest that two symptoms of CPTSD, namely, “When I am upset, it takes me a long time to calm down.” (AD1) and “I feel numb or emotionally shut down” (AD2), were the only symptoms connecting the BPD with CPTSD constructs and potentially contribute to the overlap of the two conditions (Powers et al., 2022; Frost et al., 2020)."
https://www.researchgate.net/publication/366964802_Borderline_Personality_Disorder_BPD_and_Complex_Post_Traumatic_Stress_Disorder_CPTSD_A_network_analysis_in_a_highly_traumatised_clinical_sample
"...the DSO [Disturbances of Self-Organization] symptoms of cPTSD are consistent with the flight response, which is characterized by both unmodulated distress (i.e., DSO’s difficulty in self-calming, guilt, and sense of worthlessness) and both conscious and unconscious attempts to escape from further harm (i.e., DSO’s emotional numbing and relational detachment). Flight responses involve active attempts to restore safety by disengaging from sources of harm (e.g., fear of closeness) and distress, which are highly self-referential (i.e., associated with the DMN [Default Mode Network]) and include attempts to mobilize executive problem solving and decision-making (i.e., associated with the PfC [prefrontal cortex]). Thus, cPTSD could be understood as the maladaptive persistence of initially adaptive stress reactions that progress from hypervigilance (i.e., PTSD) to emotional/relational shut-down (i.e., DSO).
BPD could emerge as a fight response when executive control capabilities are not sufficient to sustain PTSD’s freeze/hypervigilance and cPTSD’s flight/detachment, which is consistent with evidence of diminished connectivity within the salience network and the DMN, and hypoactivation of the PfC plus hyperactivation of the amygdala, in BPD. Instead of attempts to cope by means of vigilance or detachment, BPD involves reacting in a fight mode with impulsive, disorganized, and hostile behavior in relationships and limited or no sense of self-awareness and self-efficacy. The fight reaction characterizing BPD includes a surge in bodily arousal initiated by the brain’s innate alarm system [102], and desperate attempts to prevent or retaliate for perceived or real abandonment. The alternating enmeshment in and rejection of relationships characterizing BPD also is consistent with the emotional dysregulation and deficits in executive function that have been found to occur among individuals who are experiencing disorganized attachment."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8103648/
Appreciate that.
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #7 on:
May 27, 2024, 12:56:31 AM »
Quote from: Pensive1 on May 25, 2024, 08:33:32 PM
P.S. re: "what the prognosis is for someone with this degree of issues, even with therapy and medication."
I'll just comment here regarding BPD, since that seems the more relevant construct in this case.
BPD can be successfully treated. On the BPDfamily message boards, I have seen quite a lot of accounts of people who improved greatly. Certain structured therapies seem to have much greater efficacy for BPD than traditional psychotherapy. Traditional psychoanalysis "on the couch", using free-association, can sometimes cause BPD patients to deteriorate. Though even with appropriate evidence-based therapies, a substantial proportion of BPD patients show no improvement. Full recovery is possible (even in extreme cases), but appears relatively rare. Medications have very limited efficacy in treating BPD - though they can be used to ameliorate certain symptoms. But meds can't address the core problems.
DBT is the most widely used treatment for BPD. But a lot of BPD patients dislike it. Treatment dropout is frequent. I managed to engage my ex into DBT therapy, but she disliked it, showed little improvement over the course of a year and a half of therapy, and then dropped out.
Schema Therapy might currently be the most efficacious treatment for BPD. A network meta-analysis found its effect size (in reducing BPD symptoms) to be twice as large as other current BPD-specific treatments. Though that was based on a limited number of randomaized controlled trials - more research needs to be done. Schema Therapy also shows a lower patient dropout rate than other BPD therapies. One reason might be because in Schema Therapy, the therapist is often speaking to the "vulnerable child mode" in the patient (and is providing "limited reparenting"), rather than just speaking to the "adult", as in most therapies. Unfortunatetly, there are relatively few adequately trained practitioners providing Schema Therapy in the U.S., even though it was developed in the U.S. It's much more widely used in Europe and Australia.
This is good information, though if I'm reading it correctly, there's nothing definitive on how to treat it nor how well that treatment is likely to work. Am I reading this correctly?
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #8 on:
May 27, 2024, 12:59:44 AM »
Quote from: EyesUp on May 26, 2024, 06:23:30 AM
As others noted, there are some common co-morbidities, and some common features/attributes.
It does sound like your X has some b-cluster behaviors.
Ultimately, it’s up to her to accept or not accept any particular diagnosis or therapy…
From what I've read, it sure sounds like she ticks off many of the BPD boxes.
I didn't note everything she did here. For instance, she showed up in the parking lot at my job. We were on the outs then, and it wasn't a romantic thing but more like a stalker-y one. She could just never get her ex out of her life, either.
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #9 on:
May 27, 2024, 01:15:37 AM »
Quote from: Kashi on May 26, 2024, 03:45:28 AM
CPTSD has some similar traits as BPD, but it's varied depending on the individual and circumstance
What you are describing seems pure BDP to me
Anxiety can cover both BPD and CPTSD but it's a different beast.
You need to know "why"
Anxiety is so common now. From school age children all the way through. I think it's just what we as humans have come to know. Years ago we were told to suck it up take it so it wasn't spoken about.
She sounds a lot like BPD, at least according to what I've read.
Yeah, that's the thing. When we started going out regularly, she told me she had anxiety. I didn't think much of it because practically everybody I run into has got something these days. The same with ADD, etc. The worst of it then was she might get a little anxious in crowds.
As we started getting more serious, her quirks got more pronounced and unusual. She didn't like going to the movies because it was too loud and too much was going on. She got freaked out if an insect landed on her, no matter how small or benign. We'd go to a festival or do something in public she was excited about only for her to want to leave not long after we got there.
From there, things just escalated. They got stranger. Eventually, they got plain scary.
Nothing happened all at once, and getting information from her was like peeling an onion, only if the onion sometimes covered itself back up. She would say one thing, then contradict herself later. Or she'd suddenly admit to something that she'd denied weeks before.
Even with the paperwork. At one point I offered to go with her to therapy if she wanted us to work as a couple, which she said she did. But I told her I needed to understand what was going on, and the easiest way to do that was to see the diagnosis and related paperwork. By then, I'd seen what pills she was taking, and we'd discussed the rudiments, so it wasn't like everything was unknown to me.
But she waffled, saying she'd show me, then telling me it was private, and then finally producing something that, to be honest, I can't absolutely say was even legit. For all I know, she just downloaded something off the Web.
So, the "why" is in part trying to piece all this together. I was perfectly fine respecting her privacy until her problems turned into our problems and she said she wanted us to work together. Now, if I run into someone who says they have anxiety or PTSD or whatever, my reaction is to want to measure that against what I experienced to determine whether or not I want more in my life.
Logged
Kashi
Offline
What is your sexual orientation: Gay, lesb
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 91
Re: BPD? Anxiety? CPTSD?
«
Reply #10 on:
May 27, 2024, 03:17:21 AM »
I think you getting too concerned about trying to read someone to try and avoid a similar situation.
Where maybe just trust your instincts. If you need to get out do that.
My sister hates beach sand and is a bit fragile sometimes. She was always a bit strange.
BUT she is super successful and so is her husband is pretty level-headed and patient. She can be generous or a bit selfish. Depending on the day. She has so many friends it's not funny.
I understand where you are coming from but sometimes people do have weird habits or traits.
Look for the big-ticket items like do they lie, do you feel manipulated, are they independent. Stuff like that.
If the weird stuff is building up then you have a problem.
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #11 on:
May 27, 2024, 10:37:19 PM »
Quote from: HoratioX on May 27, 2024, 12:56:31 AM
This is good information, though if I'm reading it correctly, there's nothing definitive on how to treat it nor how well that treatment is likely to work. Am I reading this correctly?
There is quite a bit known about how to treat it (i.e., "there's nothing definitive on how to treat it" is not correct). But you're basically correct on the second part - how well a treatment will work for any given individual is a crapshoot.
The treatments that are known to work include (this is not a completely exhaustive list): Dialectical Behavior Therapy, Mentalization-Based Treatment, Transference-Focused Psychotherapy, Schema Therapy, DBT-PTSD, Good Psychiatric Management for Borderline Personality Disorder, and Systems Training for Emotional Predictability and Problem Solving. They are very different approaches and all have different pros and cons. These treatments produce improvements in the average patient, and all work better than "treatment as usual" (i.e., typical psychotherapy), but a lot of patients don't improve. Complete recovery appears uncommon, but does occasionally occur. An interesting case is the woman who developed DBT - she qualified for a diagnosis of BPD as an adolescent, and it was extremely severe, but she found her way out of the disorder and is now a very accomplished and celebrated therapist. Based on current data, Schema Therapy appears one of the best treatment modalities, with apparently twice the level of improvement of most other common treatments (though more research is needed to confirm this). From what I've read and heard anecdotally, a determination to improve results in better outcomes.
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #12 on:
May 29, 2024, 09:37:37 PM »
I should probably have rephrased that -- my point was that there didn't seem to a be single definitive approach versus a variety of approaches with varying degrees of success.
As I wrote, my ex was taking several medications and seeing a therapist. I don't know what specific treatments she was receiving. She generally was pretty secretive about it. Every once in a while, though, she open up a bit, usually when I was offering to work with her and her therapist, if that was possible. But for the most part, she kept me in the dark.
Interesting about the diagnosis of BPD in adolescence. I was under the impression they don't diagnose such in people under 18. I've also read conflicting things about the efficacy of treatment.
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #13 on:
May 30, 2024, 02:24:39 AM »
Quote from: HoratioX on May 29, 2024, 09:37:37 PM
Interesting about the diagnosis of BPD in adolescence. I was under the impression they don't diagnose such in people under 18. I've also read conflicting things about the efficacy of treatment.
Diagnosing BPD in individuals under age 18 used to be controversial, but that's changed. Diagnosis in adolescents was codified in DSM-V.
In case you might find Dr. Marsha Linehan's story of interest, here's a NYTimes article discussing it.
https://archive.ph/EbeNI
Traditional psychoanalysis can actually be detrimental with BPD patients.
Short excerpts from a couple articles:
"The patients that Dr. Stern was seeing appeared neurotic – with intact reality testing – on their first interview, but when they were put on the couch they got worse. Their lives unraveled and they became self-destructive as they were unable to grapple with the intense emotions that psychoanalysis brought up."
"So the prescription was classical psychoanalysis, calling for the patient to free associate while lying on the couch. "At first, she was friendly and cooperative, always on time and eager to talk about herself," Oldham recalled. "She engaged in the treatment and seemed to be benefitting from it."
A couple of months into treatment, however, the patient made an announcement. "She said to me, ‘Here I am doing just what I've always done. I blithely rush into a relationship without even thinking about it, and I don't know you at all. How do I know I can trust you?’"
She began to demand of Oldham information about himself and about his training and blamed him for what she perceived as a treatment that wasn't working. "She became convinced I was keeping secrets from her and told me the problem was that I had been trained in a ‘fly-by-night’ school," he said. "In time, she would become absolutely enraged at me, regardless of what I said. And when I didn't give her an answer she wanted, it became proof that once again she had landed in the clutches of someone who was another disappointment and who might actually harm her."
The treatment and what had appeared to be a promising therapeutic relationship ended abruptly when the patient relocated to another part of the country. For Oldham the case remains an object lesson in how not to treat a patient with BPD.
"Under no circumstances would I treat her today with psychoanalysis," Oldham said."
That's part of what I think happened with my ex. The NPD guy she's now seeing initially offered to act as her therapist (though he has absolutely no training as a therapist). They proceeded with free-association psychoanalysis, and she deteriorated. Then they began their affair. Her BPD symptoms are now far worse than in the years we were together. She believes that her "therapy" with this guy uncovered repressed material that had always been there and needed to be worked on, but the reality is that the pseudotherapy really f*cked her up. And she often does recognize that she's pretty psychologically messed up now. I did subsequently manage to engage her into proper DBT therapy (at a center that works predominantly with pwBPD), but she resisted the DBT therapy and wouldn't do the homework, and then dropped out.
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #14 on:
May 31, 2024, 11:07:27 PM »
Quote from: Pensive1 on May 30, 2024, 02:24:39 AM
Diagnosing BPD in individuals under age 18 used to be controversial, but that's changed. Diagnosis in adolescents was codified in DSM-V.
In case you might find Dr. Marsha Linehan's story of interest, here's a NYTimes article discussing it.
https://archive.ph/EbeNI
Traditional psychoanalysis can actually be detrimental with BPD patients.
Short excerpts from a couple articles:
"The patients that Dr. Stern was seeing appeared neurotic – with intact reality testing – on their first interview, but when they were put on the couch they got worse. Their lives unraveled and they became self-destructive as they were unable to grapple with the intense emotions that psychoanalysis brought up."
"So the prescription was classical psychoanalysis, calling for the patient to free associate while lying on the couch. "At first, she was friendly and cooperative, always on time and eager to talk about herself," Oldham recalled. "She engaged in the treatment and seemed to be benefitting from it."
A couple of months into treatment, however, the patient made an announcement. "She said to me, ‘Here I am doing just what I've always done. I blithely rush into a relationship without even thinking about it, and I don't know you at all. How do I know I can trust you?’"
She began to demand of Oldham information about himself and about his training and blamed him for what she perceived as a treatment that wasn't working. "She became convinced I was keeping secrets from her and told me the problem was that I had been trained in a ‘fly-by-night’ school," he said. "In time, she would become absolutely enraged at me, regardless of what I said. And when I didn't give her an answer she wanted, it became proof that once again she had landed in the clutches of someone who was another disappointment and who might actually harm her."
The treatment and what had appeared to be a promising therapeutic relationship ended abruptly when the patient relocated to another part of the country. For Oldham the case remains an object lesson in how not to treat a patient with BPD.
"Under no circumstances would I treat her today with psychoanalysis," Oldham said."
That's part of what I think happened with my ex. The NPD guy she's now seeing initially offered to act as her therapist (though he has absolutely no training as a therapist). They proceeded with free-association psychoanalysis, and she deteriorated. Then they began their affair. Her BPD symptoms are now far worse than in the years we were together. She believes that her "therapy" with this guy uncovered repressed material that had always been there and needed to be worked on, but the reality is that the pseudotherapy really f*cked her up. And she often does recognize that she's pretty psychologically messed up now. I did subsequently manage to engage her into proper DBT therapy (at a center that works predominantly with pwBPD), but she resisted the DBT therapy and wouldn't do the homework, and then dropped out.
I'm curious -- is the treatment for CPTSD similar? Generalized anxiety? Do they approach treatment from a shared perspective or so a distinct difference in how to approach the patient?
Logged
Kashi
Offline
What is your sexual orientation: Gay, lesb
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 91
Re: BPD? Anxiety? CPTSD?
«
Reply #15 on:
June 01, 2024, 04:58:56 AM »
CPTSD is a different beast. You have to get the whole family in to know what happened.
I know CPTSD very well.
I have gone through my trauma and what makes me different that BPD. Over it, through and all over it.
What makes me different when I endured, sexual abuse, a violent father, a mother who abandoned me.
There was no intermittent reinforcement of love in my life. That is the difference I see.
Where with my BPD ex there was, to the extreme. Love when pleasing, then none.
I just didn't get any. I am able to have nurturing feelings, kindness, empathy. Where did that come from?
I wasn't shown values, so I made them up. Yup. I made them up. I made up a code to live by. One that said you are strong if you don't lie. You face the consequences and it's better to do that than lie. You tell the truth to yourself even if it isn't great. You are not the sum of your past experiences unless you make it so. Your work is to slowly make yourself a better person.
There are some things that trip me up. For example, in my mind, I feel I am not supposed to be happy. If show it someone will hurt me. Because that is what happened to me. So, I practice allowing myself and the world won't implode on me if I show I am happy.
I think what has happened to them is they were handed a FIRM blueprint, where I wasn't.
The blueprint for me was I was not worthy of love the same as theirs. But I grew to believe in myself in an honest way.
Shame I allowed this person to abuse me emotionally. The intricate design of the abuse I didn't recognize.
But they do. They are replaying it just like a blueprint. It's like a map in their minds that says this is how you operate. Nothing gets them out of that.
Intermittent reinforcement is what they play out. I believe that is how they were treated as a baby.
They were given the blueprint at the start. They didn't have a chance. The brains developed with that code.
I had something very different. For example, my father was violent but never to me. To me he told me in many ways, even though you are a girl, be your own person. You can do anything. I will show you and allow you to help me build and learn. He never sexually abused me. I didn't need to please him or my mother. My mother was being abused and she needed me for emotional support. She also told me I was stupid and would never amount to anything and abandoned me.
That was the way it was. Clear cut. I knew if he walked in that door drunk, what was going to happen.
My ex her life was one of subversive bullying from both parents. She was told what pleased and what didn't, and it was random. She was told who she had to be to please her mother. She was shown her father she meant nothing, then he was a sweet kind man. Who isn't.
CPTSD BIG difference in how it played out.
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #16 on:
June 03, 2024, 01:43:12 AM »
Not sure I entirely follow all that.
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #17 on:
June 03, 2024, 07:40:24 PM »
Quote from: HoratioX on May 31, 2024, 11:07:27 PM
I'm curious -- is the treatment for CPTSD similar? Generalized anxiety? Do they approach treatment from a shared perspective or so a distinct difference in how to approach the patient?
I don't know if there's a simple answer to that. It appears that people with BPD require a very structured mode of therapy. That isn't necessarily true for people with generalized anxiety or cPTSD. Schema Therapy is a therapeutic approach that works well for BPD and multiple other conditions, including cPTSD. I think DBT, with its focus on mindfulness, can be helpful both for BPD and for cPTSD (and for other conditions as well). DBT-PTSD, a therapeutic approach developed by Martin Bohus and colleagues, was, I think, originally conceptualized as a treatment approach for cPTSD in patients with or without comorbid BPD. Then there are approaches like Mentalization-Based Treatment and Good Psychiatric Management for Borderline Personality Disorder that are specific for BPD, and that wouldn't be appropriate for a patient with cPTSD alone.
Each of these three conditions is a different thing. Though I think there's more connection/comorbidity between BPD and cPTSD, because in most cases, with either disorder, the origin is in part from childhood trauma (though trauma is not strictly required for BPD to develop). And dissociation tends to be an issue both in people with BPD and in people with cPTSD. Generalized anxiety is a pretty separate thing.
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #18 on:
June 03, 2024, 08:03:41 PM »
As I mentioned earlier, I struggle with cPTSD (and have an ex with BPD) and can relate to a lot of what Kashi says.
re: "Where with my BPD ex there was, to the extreme. Love when pleasing, then none."
The same was true with my ex. She grew up with an NPD mother and malignant NPD stepfather, and "love" was entirely conditional. It was only received when she pleased them. Moreover, there was a scarcity of parental love, and only one of the siblings could be "loved" at a time, creating a lot of jealousy and dysfunction between the sibs.
re: "One that said you are strong if you don't lie. You face the consequences and it's better to do that than lie. You tell the truth to yourself even if it isn't great."
Likewise, truth is
extremely
important to me, to an unusual degree. I think that helped keep me sane.
re: "I feel I am not supposed to be happy."
I can relate to this too. And a negative self-image is pretty universal in people with cPTSD.
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #19 on:
June 04, 2024, 08:52:25 PM »
Quote from: Pensive1 on June 03, 2024, 07:40:24 PM
I don't know if there's a simple answer to that. It appears that people with BPD require a very structured mode of therapy. That isn't necessarily true for people with generalized anxiety or cPTSD. Schema Therapy is a therapeutic approach that works well for BPD and multiple other conditions, including cPTSD. I think DBT, with its focus on mindfulness, can be helpful both for BPD and for cPTSD (and for other conditions as well). DBT-PTSD, a therapeutic approach developed by Martin Bohus and colleagues, was, I think, originally conceptualized as a treatment approach for cPTSD in patients with or without comorbid BPD. Then there are approaches like Mentalization-Based Treatment and Good Psychiatric Management for Borderline Personality Disorder that are specific for BPD, and that wouldn't be appropriate for a patient with cPTSD alone.
Each of these three conditions is a different thing. Though I think there's more connection/comorbidity between BPD and cPTSD, because in most cases, with either disorder, the origin is in part from childhood trauma (though trauma is not strictly required for BPD to develop). And dissociation tends to be an issue both in people with BPD and in people with cPTSD. Generalized anxiety is a pretty separate thing.
I find it interesting -- and more than a bit confusing -- that she was diagnosed with three different issues by three different therapists. Now, again, that's if I take her at her word. She might well have been deceiving me about all that, too.
What I sometimes wonder is if a really clever and devious psychopath or sociopath could learn about these illnesses and then mimic the behaviors. My ex qualified for disability, for instance, because of her issues, but she also seemed to get enormous sympathy, as well as access to any number of medications (some of which she sold). Given how deceptive people with, say, BPD can be, it's rather disturbing. There were times when I felt genuine menace coming from her.
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #20 on:
June 05, 2024, 01:24:42 AM »
Quote from: HoratioX on June 04, 2024, 08:52:25 PM
I find it interesting -- and more than a bit confusing -- that she was diagnosed with three different issues by three different therapists. Now, again, that's if I take her at her word. She might well have been deceiving me about all that, too.
That's not necessarily too surprising. Therapists can be fallible, and a lot of practicing therapists lack good diagnostic skills. And honestly, there are many really flakey therapists out there - one licensed therapist I knew believed that mental illness was caused by radiation, and if she had a Geiger counter that she could use to check if people were emitting radiation, she could prove it.
And many people with BPD, especially those that are somewhat higher functioning, can initially present in a way where the BPD is not obvious. On top of that, there's still some confusion and overlap in the professional literature between descriptions of cPTSD and BPD, and there's a lot more confusion between these two in material that you can find online written by nonscientists. And as you mentioned, some therapists don't like to diagnose a patient with BPD because of the associated stigma (including because of concern that the patient may react badly to such a diagnosis).
My ex has BPD - very clearly meets the DSM-5 criteria (as well as other indicators described in the medical literature that aren't included in the current DSM definition). But she's never been properly diagnosed. She tells people she has cPTSD because she hates the stigma associated with BPD (she was never actually diagnosed with cPTSD). She actually trained as a therapist years ago, and the horror stories she heard from instructors about BPD clients (and this was before there was any valid established treatment for BPD) makes her especially averse to a BPD diagnosis. She recently attended DBT therapy, for a year and a half, where everyone else in her therapy group had a diagnosis of BPD, and she's still resistant to applying that label to herself - though it's clear to me from some things she says that part of her does recognize that it's the correct diagnosis.
Logged
jaded7
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Romantic partner
Relationship status: unclear
Posts: 592
Re: BPD? Anxiety? CPTSD?
«
Reply #21 on:
June 05, 2024, 11:00:24 AM »
Quote from: Pensive1 on June 05, 2024, 01:24:42 AM
And many people with BPD, especially those that are somewhat higher functioning, can initially present in a way where the BPD is not obvious. On top of that, there's still some confusion and overlap in the professional literature between descriptions of cPTSD and BPD, and there's a lot more confusion between these two in material that you can find online written by nonscientists. And as you mentioned, some therapists don't like to diagnose a patient with BPD because of the associated stigma (including because of concern that the patient may react badly to such a diagnosis).
My ex has BPD - very clearly meets the DSM-5 criteria (as well as other indicators described in the medical literature that aren't included in the current DSM definition). But she's never been properly diagnosed. She tells people she has cPTSD because she hates the stigma associated with BPD (she was never actually diagnosed with cPTSD). She actually trained as a therapist years ago, and the horror stories she heard from instructors about BPD clients (and this was before there was any valid established treatment for BPD) makes her especially averse to a BPD diagnosis. She recently attended DBT therapy, for a year and a half, where everyone else in her therapy group had a diagnosis of BPD, and she's still resistant to applying that label to herself - though it's clear to me from some things she says that part of her does recognize that it's the correct diagnosis.
All of this resonates with me. As I mentioned elsewhere, my ex needed to have a 'really important' conversation with me early on, to tell me she had cPTSD from her abusive marriage. She later mentioned things like hypervigilance and inability to be vulnerable, but not to me so much as to other people. We never had a real discussion of her 'cPTSD' and its effects on our relationship.
She also told me that she saw someone for EMDR, and that cured her....but then she'd maintain that she still had cPTSD.
After the ending is when I really started to look at all this to try to make sense of her behavior. She had explosive anger, was always assuming bad intentions on my part when I offered to help her with something- these two things went together-, was really edgy when I was at her house and I had to be careful about everything I did there.
Honestly, I don't know what her issue was. As others have said her many times, perhaps the 'diagnosis' isn't important, the behavior is:
explosive anger, name calling, hanging up the phone mid conversation, finger pointing in face, violently pulling off the highway and threatening to kick me out of the (my) car, belittling, sarcasm, contempt, ignoring texts and calls for days, mind reading expectations, cutting me off in arguments, lies and gaslighting, controlling behaviors all over the place, put downs, withholding, judgement, anger and snapping in sex, serious anger if I said no to sex, blowing through boundaries and explicit 'no's.
The behavior is probably enough to just say this is abusive and unloving.
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #22 on:
June 05, 2024, 10:44:26 PM »
Interesting -- I've read many posts on this board and elsewhere where people say that BPD symptoms or behaviors are screamingly obvious once you know what to look for. For instance, people talk about a kind of dissociative stare or point out how people with BPD frequently lie or misremember things. But then I also see a fair number of posts where people say the symptoms or behaviors are much more subtle, to the degree that therapists can have a hard time diagnosing them.
That seems contradictory. No, I don't expect everyone with BPD to have precisely the same symptoms or behaviors nor to the same degree. But the degree of distance between screamingly obvious and much more subtle seems pretty far.
I think this is one of the reasons it's tougher to figure out what happened after a breakup with someone who might have BPD (or presumably CPTSD or anxiety when the symptoms and behaviors seem similar).
That just seems to add to the confusion.
Logged
Pensive1
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: broken up
Posts: 122
Re: BPD? Anxiety? CPTSD?
«
Reply #23 on:
June 05, 2024, 11:59:39 PM »
BPD is, to a major degree, a psychological disorder that plays out around relationships. Many people with BPD can function reasonably well in contexts that don't involve close personal relationships (for example, in a workplace). In many contexts, the symptoms can be somewhat minimal. Often, with therapists, the BPD will emerge as the therapeutic relationship progresses. Just a week ago, my own current therapist (who has many decades of experience) mentioned to me that she'd had a client where she didn't detect the BPD initially, but where it ultimately became very clear.
I'll also note that with BPD, cPTSD, and anxiety disorders, there can be comorbidity. One condition might be diagnosed, while missing another.
Another things that complicates diagnosis is that people with other mental health disorders can manifest some of the symptoms of BPD. For example, my ex-wife has bipolar disorder and suffered some childhood trauma, and she would engage in splitting (as occurs in BPD).
I'll also mention - and this wouldn't apply so much with therapists - that denial can play a role in not recognizing BPD. That's true of myself, regarding my ex. My mother had BPD, and my childhood was incredibly difficult because of it. But, despite 25 years together, I didn't recognize that my ex had BPD until after she monkeybranched, and my therapist pointed it out. I even initially argued with my therapist when she noted it. But after my denial faded, it was so clear, and I couldn't believe that I hadn't recognized it. I always knew that my ex had major mental health issues (and I occasionally joked with friends that I'd gone from my ex-wife, who had bipolar disorder, to someone with even worse psych issues), but I hadn't recognized the BPD - ascribing the problems to depression, ADHD, anxiety, etc. Probably part of why I didn't recognize it was because it manifested somewhat differently than in my mother. But from the beginning I realized that she was very needy (like my mother) and was overflowing with tales of victimization and resentment (like my mother), and I was pretty allergic to both those things, given my childhood. But other symptoms played out differently (e.g., my ex would do helpless waif needing constant rescue, and my mother never did that). And my ex didn't really lie much (though misremembering was a major problem, and, more recently, she's exhibited frank dissociative amnesia).
The behaviors you listed in the original post read like a list of BPD symptoms.
I think the more exposure someone gets to people with BPD (with a large enough sample size), the better they can get at recognizing it (even when it's manifesting in somewhat different ways).
Logged
HoratioX
Offline
What is your sexual orientation: Straight
Who in your life has "personality" issues: Ex-romantic partner
Relationship status: Broken Up
Posts: 144
Re: BPD? Anxiety? CPTSD?
«
Reply #24 on:
June 06, 2024, 09:10:37 PM »
Lots of good responses in this thread, but yours here was particularly so.
Diagnosing these various illnesses seems a lot more like an art than in physical medicine (which I understand isn't a black-and-white thing either). I think my ex definitely ticked off many boxes for BPD, including others I didn't list.
That bit about denial is particularly interesting. As with a lot of people who had relationships with people with BPD (etc.), my instincts told me something was off right away. The first time I met her, I thought she was flighty and a little clumsy, like Suzanne Somers in Three's Company. Her voice sounded breathy, like Marilyn Monroe's. It all seemed charming, maybe immature, but at the same time, unusual.
As the relationship went on, I saw clear red flags, but then, after having been in my share of relationships, I thought of how often I'd misread or not been patient enough with my girlfriend's before, where I'd not been generous enough to take their wants and needs better into account. So that made me, I think, more determined to try to work things out with this one. And, of course, not being familiar with BPD, CPTSD, or anxiety (in a clinical sense), I had no real idea of the territory I was in. I was still thinking on some level that I was dealing with someone who operated in a rational way, even if her personal style was a little kooky.
It was all a perfect storm to be in something that went on much longer than it should have.
Nonetheless, I think there was a degree of denial to that, especially in the sense of not taking the red flags 100% for what they were. At the same time -- and I know this might sound like rationalization -- I do think there were some mitigating factors. Once all that worked itself out in the fog of a chaotic relationship where I would eventually discover the girlfriend routinely lied, cheated, or deceived, then the need for the break up was clear. It took time for all that to happen, but once it did, I took action and haven't gone back. But if I'd trusted my instincts more to begin with, I could have avoided a lot of the suffering (though I suppose I might have had more regrets if I hadn't yet confirmed everything).
I do know I'll be more aware if I ever cross paths with someone like this again and that I'll trust those instincts a lot more.
Logged
Can You Help Us Stay on the Air in 2024?
Pages: [
1
]
Go Up
Print
BPDFamily.com
>
Relationship Partner with BPD (Straight and LGBT+)
>
Romantic Relationship | Detaching and Learning after a Failed Relationship
> Topic:
BPD? Anxiety? CPTSD?
« previous
next »
Jump to:
Please select a destination:
-----------------------------
Help Desk
-----------------------------
===> Open board
-----------------------------
Relationship Partner with BPD (Straight and LGBT+)
-----------------------------
=> Romantic Relationship | Bettering a Relationship or Reversing a Breakup
=> Romantic Relationship | Conflicted About Continuing, Divorcing/Custody, Co-parenting
=> Romantic Relationship | Detaching and Learning after a Failed Relationship
-----------------------------
Children, Parents, or Relatives with BPD
-----------------------------
=> Son, Daughter or Son/Daughter In-law with BPD
=> Parent, Sibling, or In-law Suffering from BPD
-----------------------------
Community Built Knowledge Base
-----------------------------
=> Library: Psychology questions and answers
=> Library: Tools and skills workshops
=> Library: Book Club, previews and discussions
=> Library: Video, audio, and pdfs
=> Library: Content to critique for possible feature articles
=> Library: BPDFamily research surveys
Our 2023 Financial Sponsors
We are all appreciative of the members who provide the funding to keep BPDFamily on the air.
12years
alterK
AskingWhy
At Bay
Cat Familiar
CoherentMoose
drained1996
EZEarache
Flora and Fauna
ForeverDad
Gemsforeyes
Goldcrest
Harri
healthfreedom4s
hope2727
khibomsis
Lemon Squeezy
Memorial Donation (4)
Methos
Methuen
Mommydoc
Mutt
P.F.Change
Penumbra66
Red22
Rev
SamwizeGamgee
Skip
Swimmy55
Tartan Pants
Turkish
whirlpoollife
Loading...